The medical community continues to strive for advancements in diagnostic technologies, particularly those that can detect pathogens directly from blood samples. A recent session at ASM Microbe 2024 in Atlanta chaired by Linoj Samuel delved into the complexities and challenges that have hindered the integration of these technologies into clinical practice. Direct-from-blood pathogen detection technologies are designed to bypass traditional culture methods, which can be time-consuming and sometimes ineffective in identifying fastidious or non-culturable pathogens. By utilizing such tools, healthcare providers can obtain actionable information swiftly, allowing for the narrowing of therapy and de-escalation of antibiotics. This rapid turnaround is crucial in managing sepsis, where every hour counts in the race against mortality and morbidity.
The session highlighted a blend of technical and non-technical challenges, from the intricacies of sample preparation, pathogen detection to the broader implications for clinical decision-making. Dr. Valeria Fabre’s insightful presentation underscored the potential of these technologies to revolutionize patient care, offering a clinician’s perspective on their impact on treatment strategies.
Economically, the implementation of these technologies presents both challenges and opportunities. While initial costs may be higher due to equipment and workforce training, the potential for reducing the length of hospital stays, decreasing the use of broad-spectrum antibiotics, and preventing the spread of resistant pathogens lead to significant savings.
Key takeaways from the discussion emphasized the need for a deeper understanding of the goals behind direct-from-blood pathogen detection. What are the specific outcomes we aim to achieve? How can these technologies influence clinical decisions, patient outcomes, and the economic aspects of healthcare? The current absence of this information hinders assessment of the value such diagnostics bring and thus their adoption. While much of the current efforts are focused on nucleic acid technologies, the development of imaging and spectroscopy-based technologies adds to the diversity of diagnostic approaches, potentially offering complementary benefits to nucleic acid-based methods. These technologies may provide additional layers of information, that may not be available through nucleic acid testing, such as greater confidence in detecting the presence/absence of bacteremia and antimicrobial susceptibility information.
Overall, there is a palpable sense of optimism about the future. The next generation of pathogen detection technologies promises to address current technical limitations more effectively. However, the adoption of these technologies hinges on a much better understanding, and more importantly demonstration, of their value. Failure to take this into account during development and design of validation studies may inhibit their use in clinical settings, which would be a shame.
Many recent articles have called for overhauling antibiotic pricing as one of the key ways to lure investments in antibiotic development. But, its beneficial effects, in my opinion, are exaggerated.
Alarm bells are being rung with several articles over the last few weeks in the Wall Street Journal, New York Times, and The Washington Post (to name a few) discussing how challenging the climate is for antibiotic developers. Many quoted in these articles call for an overhaul of antibiotic pricing with the central thesis being that such an overhaul will provide much needed revenue and attract investment for struggling antibiotic developers, thus recharging the efforts to combat the antimicrobial crisis. But, will it?
Past efforts to increase drug prices generated a lot of opposition and much hand wringing (see infographic). Those objections were however generally directed towards very expensive cancer drugs or overpricing of drugs. But the fundamental reasons for the opposition have not disappeared.
Certainly, antibiotic developers are struggling. They do not earn anywhere close to the revenue that a successful cancer therapeutic developer would and these struggles are well documented. But what will increasing the price/reimbursement of an antibiotic really do? The thinking goes that if antibiotic developers are successful, it will draw in more money and talent creating a virtual cycle that will be self-sustaining.
But, is it self-sustaining and will it achieve its desired goals? Everyone acknowledges that the two key reasons why antibiotic developers struggle are because (a) hospitals prescribe these new drugs sparingly to avoid building up resistance to them and (b) they try a lower cost alternative first.
When decisions on which antibiotic to use are still based entirely on clinical judgment, i.e. a good educated guess, going with the lower cost option or hoarding a “drug of last resort” is logical and natural. Why do we think that increasing reimbursement will alter this behavior. And unless we do something that changes this dynamic we are not really solving the problem. We are just creating a new special interest.
Antibiotics are the lifeblood of modern medicine. And antimicrobial resistance is a global problem. If the price of the antibiotic were raised, will other countries break patents invoking “national emergencies” much as was done to get inexpensive HIV drugs?
If the drugs are inexpensive in, say India, and are used extensively there because they work, how long do you think it will be before resistance develops for these drugs?
If you went to a physician and after a visual examination, the physician recommends that you undergo cancer treatment because he/she suspects you have cancer, would you do it or would you change physicians? But, this is what we do every single day with infections and antibiotics. And if someone comes along saying the solution is to have pricier drugs, well…
Look, I get the point about reviewing pricing of antibiotics to aid discovery and development of new drugs. They need help. But, these can be one-time efforts. But, overhauling reimbursements of drugs (which sets up a long-term impact) is not the answer to combating antimicrobial resistance. It is not sustainable and will do nothing to change prescribing behaviors. When we can assure appropriate usage of antibiotics, we can influence prescription behavior and then revenues will take care of themselves.
Aha! So how do we assure appropriate usage of antibiotics? The only way I am aware of is by having a diagnostic that can truly guide treatment decisions along with improved awareness and preventive measures that hospitals are already beginning to take. If such a test were available, then physicians would not hoard. They would not try the lower cost option just because it is there. But they will pick the drug because it will provide maximum benefit to the patient. And because we will not be overusing or misusing the antibiotic, resistance spread will be slower. Note that all of these benefits can be achieved without raising drug pricing. So I would say that we should be redoubling efforts to ensure appropriate usage of antibiotics (especially new antibiotics) that meet the needs of hospitals, physicians, and patients and not fiddling with drug pricing.
You might say my position is biased because of my affiliation. It is not. But, the best way to counter my argument would be to provide a better self-sustaining model – one that helps developers, patients, and the healthcare system. Overhauling pricing helps the developers directly and very tenuously, the patients, healthcare system, or society. And as much as I relate with drug developers (having been one), such a strategy (increasing pricing/reimbursements) does not make for good policy.
New Year’s greetings and best wishes for 2020 to all!
We had ended last year, coincidentally, pondering why wide spread application of PCR-based tests in bacterial diagnostics has been elusive and identified a couple of key features that limit their use. It seems appropriate to start the new year with a discussion on one technology that can address those limitations – Infrared-based identification (IR).
What, you might be wondering, – that dilapidated instrument I vaguely recall using in undergraduate chemistry lab? Well, not quite that instrument but yes, one that utilizes the same fundamental principles.
The concept of using IR for identifying bacteria is not new. The earliest reference that we have been able to find dates back to 1950s! But, instrumental and computational limitations held back the potential for using this technology for identifying bacteria until the early 1980s. Naumann and colleagues took advantage of computational advances to demonstrate the ability of this technology to identify bacteria rapidly. Since then the use of IR for rapid and reliable identification of microbes to the strain level have been well documented. Reference databases to facilitate rapid identification of microorganisms are already available with some containing as many as 7000 strains.
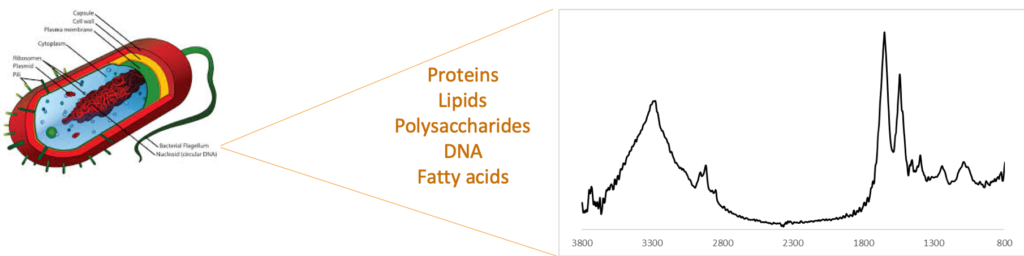
How does the technology work? IR, as you may recall, is a widely used vibrational spectroscopy technique that is used to identify compounds, even those present in mixtures. It is routinely used in raw material testing in the pharmaceutical and other industries as well as in testing of milk and milk products. All of the components that make up a bacterium (proteins, lipids, sugars, etc.) contribute to an IR “fingerprint” (see figure below). The nature and concentration of these components differ from one strain to another resulting in unique IR-fingerprints. This bacterial fingerprint has been used to differentiate between multiple bacterial species and strains including differentiating between antibiotic-resistant and -susceptible strains.
Bacterial fingerprint obtained by Infrared spectroscopy. Each species and strain has a different composition and hence a unique fingerprint.
How does it compare to PCR-based identification? Two key limitations of PCR-based tests that we had discussed previously were clinical sensitivity of the test and cost per test. If a PCR-test yielded a negative result, the clinician would not have any actionable information. On the other hand, with IR-based identification, the profile of a bacteria is very distinctive and its absence clearly indicates the absence of bacteria in the sample. In such a case, the clinician can actively consider whether administering antibiotics will be of any benefit to the patient. In the case of a positive result, the actions are similar to that with a PCR-based test with several important benefits. These are:
the result is available in ≤ 10 minutes
No custom labels or reagents are needed lowering the cost per test
It does not require specialized laboratory for operation
The bacteria is intact and viable after the analysis
Antibiotic resistance can be determined
The number of species and strains that are identified can be easily expanded without requiring new primers or antibiodies. This is done as a software update that consists of the fingerprint of the new bacteria and adjustments to the recognition algorithm, if needed.
You might be wondering at this stage why, if IR has all these benefits, there has not been any IR-based commercial instrument for use in bacterial ID? There are commercial instruments from Bruker, Thermo, and others that are used for bacterial ID in food safety testing. However the methodology used today requires bacteria to be cultured prior to identification (i.e. the same as most PCR-based tests). In addition, the bacteria has to be separated from the matrix components in order to make an accurate ID. Owing to these reasons, the technology has not yet seen widespread adoption for clinical use.
It is this aspect that we have impacted with the development of our separation cartridge. As mentioned previously, our separation cartridge can isolate and concentrate intact bacteria directly from blood with minimal manual intervention. The isolated bacteria can be identified using any technique. Using it upstream of IR however, permits rapid and sensitive identification of bacteria directly from patient sample without using any bacteria-specific labels or reagents. This combination of our separation cartridge and IR-based identification will, we believe, permit rapid, inexpensive, and hypothesis-free detection and identification. We aim to demonstrate this in 2020.
As we have said before, it’s not that IR (or any other ID technique) has to wholly replace PCR-based tests. The problem is large enough that multiple solutions will be needed. But, given the history of limited gains in developing effective PCR-based bacterial ID tests, the more diagnostic options we have, the better we can aid physicians in making the best decisions for treatment while slowing the spread of antimicrobial resistant bacteria. IR-based identification presents a compelling case to be a key diagnostic option.
A common refrain in this post-antibiotic era is that we need new antibiotics and new diagnostics . While the challenges of developing a new antibiotic are better acknowledged and understood, many are very surprised that we still use fundamentally the same procedure as used pre-WWII.
So, how is it that we are, at the start of 2020 and ~30 years since the dawn of the PCR-era, still talking about the need for better bacterial diagnostics? There are multiple technical and real-world challenges that continue to stymie the development of PCR-based tests such as speed, volume that can be processed, number of bacteria identified, and so on. Sensitivity and Specificity of a PCR-based test (or rather the lack of sufficient Sensitivity and Specificity) are two key performance attributes that have held back widespread clinical use of PCR-based tests. For this discussion, we focus on identifying bacteria directly from blood for guiding treatment of bloodstream infections, especially those that might lead to severe sepsis or septic shock.
Multiple PCR-based approaches are being developed to rapidly identify bacteria from blood. To a neutral observer it would appear that the reason we do not have a suitable bacteria test is because we have not developed a good enough PCR-based test. And that suitably optimizing such a test would solve the problem. Is this correct? Or are there some fundamental limitations that have held back clinical application?
In our opinion, the fundamental technical limitation is centered around the sensitivity of PCR-based tests and a fundamental practical limitation is centered around the ability to lower costs to a level that the healthcare system can support.
There are numerous text books and reviews providing a basis for determining the sensitivity and specificity of a test. Here is one. Briefly, Sensitivity refers to how good a test is at correctly identifying people who have the disease. While Specificity is concerned with how good the test is at correctly identifying people who do not have the disease.
What can we learn from these numbers for a bacterial diagnostic based on PCR? Let’s take the case of a hospital that analyzes 100,000 bacterial ID tests a year.
The percentage of samples that turn positive upon blood culturing ranges from 5 to 10%. Using the upper end of this range it means that out of the 100,000 samples submitted for bacterial ID tests, ~10,000 turn positive. [Note: This is frequently viewed as the number of samples that actually contain bacteria though there is widespread acknowledgment that culturing underestimates the number. More on this later. But, for the moment, since culturing is the gold standard (albeit an imperfect one) let’s go with 10,000 samples out of the 100,000 samples contain bacteria and therefore represent an infection.]
Data from two commercially available PCR based tests exhibit sensitivity and specificity are shown in the table below.
Sensitivity
Specificity
Septifast ®
42.9%
88.2%
SepsiTest ®
28.6%
85.3%
The sensitivity of these two tests range from 28.6% to 42.9%. In other words, if the PCR result came back negative (suggesting there is no bacteria), you could only be ~43% sure that there really was no infection! Think about that for a moment. If you were a physician making this decision, would you decide not to administer antibiotics based on this result? You’re most likely going to administer the antibiotics as you’re not that confident that you can rely on the negative result. Similarly, the specificity of these two tests range from 85.3% to 88.2%. In this case, you can be 88% sure that if you got a positive result, the patient has an infection though there’s a 12% chance that the result may not be accurate.
Let’s apply the above numbers to our hospital that processes 100,000 blood culture samples. Suppose that these samples are tested by a PCR-based test instead of being submitted for blood culture testing. Using the Sensitivity and Specificity numbers from above, this means that, of the 100,000 samples, 15,400 will yield a positive result. But, only 4,600 of these are truly positive. So, you will end up administering antibiotics unnecessarily for a large number of patients based on the 10,800 positive results. Similarly, you would have had 84,600 negative results of which 5,400 are false negatives. This means that you would have chosen not to administer antibiotics despite patients needing it.
“True” Result
Positive
Negative
PCR test positive
4,600
10,800
PCR test negative
5,400
79,200
As a physician or a hospital, the number of incorrect decisions resulting by relying on such a test is too high – jeopardizing patient safety. Does it really provide a significant benefit over the current practice where antibiotics are administered based largely on clinical judgment? At the present moment at least, the general opinion is no. Since it does not offer significantly helpful guidance relative to current practice it does nothing to correct overuse or misuse of antibiotics.
Most of the time when we consider how to use the result from a diagnostic test, we ask ourselves, if it yields a positive result would I know what to do next? That is an important question. But, in this application, it is equally (if not more) important to ask if the test yields a negative result, would I know what to do next? There is not sufficient data (and may never be) to guide treatment decisions when a PCR-based test is negative. This is the fundamental technical limitation.
Besides their performance, PCR-based tests also create problems due to their cost and operation. A single test costs $70 – $200 based on the number of bacteria identified. Using our example, if such a test were used for each sample currently submitted for blood culture, it would cost each hospital $7-$20 million (just in consumables). Which consumes a significant portion of a microbiology lab budget leaving little to no money for other tests. And still leaves a large number of bacteria unidentified!
In theory one can design a PCR test that is multiplexed to cover a large number of bacteria. But, this will increase the cost per test. Splitting the number of bacteria identified across multiple test panels is one way of covering a broader range. But, this takes away the advantages of cost reduction due to large volumes. How does one respond to new strains or species that are of urgent concern that was not anticipated? In different regions of the world? The modifications to the manufacturing process to address these different demands make it very challenging for the manufacturer to keep costs low.
So, at a fundamental level, PCR-based tests for identifying bacteria directly from blood face limitations due to poor performance, high costs, and appear to not aid decision-making or operational efficiency.
Significantly improving sensitivity and controlling costs are therefore necessary, but not sufficient, conditions for enabling widespread use of PCR as a bacterial ID test direct from patient sample. And until they are satisfactorily resolved, there will continue to be a reluctance in using such tests to guide antibiotic treatment.
Which means that we owe it to ourselves and all patients to consider and develop alternative ID techniques. It’s not that one technique is a winner and the other the loser in such an effort. The problem is large enough that multiple solutions will be needed. The more diagnostic options we have, the better we can aid physicians in making the best decisions for treatment while slowing the spread of antimicrobial resistant bacteria.