The medical community continues to strive for advancements in diagnostic technologies, particularly those that can detect pathogens directly from blood samples. A recent session at ASM Microbe 2024 in Atlanta chaired by Linoj Samuel delved into the complexities and challenges that have hindered the integration of these technologies into clinical practice. Direct-from-blood pathogen detection technologies are designed to bypass traditional culture methods, which can be time-consuming and sometimes ineffective in identifying fastidious or non-culturable pathogens. By utilizing such tools, healthcare providers can obtain actionable information swiftly, allowing for the narrowing of therapy and de-escalation of antibiotics. This rapid turnaround is crucial in managing sepsis, where every hour counts in the race against mortality and morbidity.
The session highlighted a blend of technical and non-technical challenges, from the intricacies of sample preparation, pathogen detection to the broader implications for clinical decision-making. Dr. Valeria Fabre’s insightful presentation underscored the potential of these technologies to revolutionize patient care, offering a clinician’s perspective on their impact on treatment strategies.
Economically, the implementation of these technologies presents both challenges and opportunities. While initial costs may be higher due to equipment and workforce training, the potential for reducing the length of hospital stays, decreasing the use of broad-spectrum antibiotics, and preventing the spread of resistant pathogens lead to significant savings.
Key takeaways from the discussion emphasized the need for a deeper understanding of the goals behind direct-from-blood pathogen detection. What are the specific outcomes we aim to achieve? How can these technologies influence clinical decisions, patient outcomes, and the economic aspects of healthcare? The current absence of this information hinders assessment of the value such diagnostics bring and thus their adoption. While much of the current efforts are focused on nucleic acid technologies, the development of imaging and spectroscopy-based technologies adds to the diversity of diagnostic approaches, potentially offering complementary benefits to nucleic acid-based methods. These technologies may provide additional layers of information, that may not be available through nucleic acid testing, such as greater confidence in detecting the presence/absence of bacteremia and antimicrobial susceptibility information.
Overall, there is a palpable sense of optimism about the future. The next generation of pathogen detection technologies promises to address current technical limitations more effectively. However, the adoption of these technologies hinges on a much better understanding, and more importantly demonstration, of their value. Failure to take this into account during development and design of validation studies may inhibit their use in clinical settings, which would be a shame.
Isolating bacteria directly from blood or positive blood culture present a unique set of problems for clinical microbiologists and researchers. We are happy that multiple recent studies using our Separation Cartridge have performed very well in both applications. This post relates to the positive blood culture application.
One ongoing study at a local hospital has observed that traditional ID results could be obtained within a day (whereas without using the cartridge results have taken 2-5 days) and that the ID results obtained using the cartridge matches that obtained by subculturing.
The shorter time-to-result using the cartridge was because it eliminated the need for subculturing decreasing the time to ID & AST by at least 24 hours. While it is generally accepted that that direct testing of positive blood culture broths is feasible, results have been variable (for instance better success with Gram-negative rods (GNR) than Gram-positive cocci (GPC)), workflow sub-optimal, or the method too expensive.
Preliminary experiences indicate that the cartridge does not have these limitations. The process takes ≤ 5 minutes, requires no new instrumentation, and uses one buffer that can be easily sourced. Results have been consistent regardless of whether it is GNR / GPC. More studies are taking place at other hospitals and microbiology labs that we will keep you updated on.
If this is an area of interest to you or your organization, please contact us (www.3idx.com). We are interested in setting up demos and additional studies to assess performance in different settings and applications. Thank you.
The Seventy-fifth World Health Assembly is being held in Geneva, Switzerland, from May 22-28, 2022. It is the first in-person Health Assembly since the start of the COVID-19 pandemic. On the occasion of the start of this assembly, many health-related organizations have released statements on healthcare priorities, inequities, and focus for the future.
Some of these observations relating to diagnostics caught our attention. We list four of them below and see them as further motivation for the work that we are doing at 3i Diagnostics.
The capacity to perform basic tests is available in just 1% of primary care clinics in low- and middle-income countries.
No diagnostic tests exist for 60% of the pathogens identified by the World Health Organization (WHO) as having the greatest outbreak potential. There are also no appropriate tests for half of the top 20 diseases responsible for the most lives lost.
Using COVID tests as an example, high-income countries use COVID tests at 10–100 times the rate of middle- and low-income countries. So, if tests are not inexpensive, testing is likely to be deficient.
Early diagnosis has been consistently linked to improved health outcomes and reduced out-of-pocket spending. However, diagnosis is the weakest link in healthcare systems globally.
One of the key learnings from COVID-19 is that investing in diagnostics will be central to rapid response to outbreaks and delivering appropriate care for infections. Deficiencies in testing affect not only people’s lives, but communities and economies, as COVID-19 clearly showed.
There has been a notion among many in the medical community that a significant proportion of the morbidity and mortality associated with COVID-19 are due to secondary bacterial infections. This notion is, in part, attributed to studies from the 2009 H1N1 epidemic (Morris et al. ) , and early reports detailing increased presence of other respiratory pathogens in COVID-19 patients (Gerberding , Zhou et al. , Zhu et al. ). Accordingly treatment of COVID-19 patients have frequently included antibiotics.
As Andrew Jacobs reported in his New York Times article, physicians heavily prescribed antibiotics for treating these patients because of this concern. It now appears that this possibility is not as pervasive or as severe as initially thought (Rawson et al.).
While the fear of opportunistic infections have not come to pass, the overuse of antimicrobials in treating COVID-19 patients has highlighted concerns about catalyzing a slower-moving crisis namely antimicrobial resistance (AMR). Overuse of antibiotics is one of the factors that induces the development of resistance and its spread, which is precisely what we have done over these past few months.
What is interesting is that in both situations, COVID-19 and AMR, the immediate challenge has been our inability to identify those patients who need urgent medical attention. The challenges in testing subjects to determine if they are COVID-positive or not are well documented. Less well recognized is the situation in tackling AMR.
In the case of AMR, while much attention has been devoted to developing new drugs, as they should, the fact is that the fundamental problem is that we do not know which drug to administer to treat the patient efficiently and rapidly. That is, it is at heart a diagnostic problem. As the US Government Accountability Office succinctly explain in their assessment of US efforts to combat AMR “Without information to guide test usage, clinicians may not be able to select appropriate treatments for their patients.”
If you think that waiting for 48-72h to know if you were COVID-positive was unacceptable, why should it be for detecting bacterial infections, which could be just as, if not more, deadly (e.g. Sepsis)? [Today, it takes 1-5 days before the physician can learn if the patient has a bacterial infection or not] As Dr. Strich of the NIH clinical center is quoted as saying, “being prepared is more cost effective in the long run” and saves lives. “Antimicrobial resistance is a problem we cannot afford to ignore.”
And yet, there is not the same sense of urgency in developing diagnostics that can rapidly determine if a patient has a bacterial or vial infection let alone what the infection-causing pathogen is. Efforts to develop better diagnostics are not sufficiently supported by either the private or the public sectors.
We should all be asking ourselves why we are not pushing, with a greater sense of urgency, for better diagnostics that will be effective in combating AMR or the next pandemic instead of just hoping that the same approaches that have been tried for 20+ years with limited success will somehow suddenly provide the solution?
These are challenging times, and we, at 3iDx, hope that you, your loved ones, friends, and colleagues are well.
The COVID-19 pandemic has impacted the world in ways not seen in modern times. One of these is to bring back the importance of diagnostics and, importantly, the ability to perform tests in a multitude of settings.
It is abundantly clear that controlling the outbreak through social distancing severely impairs a functioning society. Any strategy to “reopen” a country is highly reliant on better testing, which is central to reducing transmission and morbidity and mortality. This not only involves being able to obtain an actionable result but also encompasses producing tests at a scale commensurate with the outbreak and addressing massive challenges in the supply chain.
While DNA-based diagnostic testing offers several reasons to include in our armament of tools. Waiting multiple hours or even days before getting a result for a COVID-19 test does not strike one as an effective strategy especially when battling reagent and buffer shortages.
While high-income countries are facing challenges in meeting the diagnostic needs of their rural and semi-urban populations, these challenges are magnified in low- and middle-income countries. These countries currently have the lowest rates of testing reported to the WHO.
It feels strange to be listing these problems and areas for improvement in yet another global crisis. We had earlier observed how our response to the antimicrobial resistance crisis is being held back because of inadequate diagnostics. The needs in both crises are eerily similar. We need rapid and inexpensive diagnostics that can be scaled easily and used outside a specialized laboratory setting. The options we currently have are not it.
The current COVID-19 crisis will draw down and we will emerge stronger. But if we are to emerge wiser from this experience, we need to invest more (resources, attention, capital) in diagnostic development.
New Year’s greetings and best wishes for 2020 to all!
We had ended last year, coincidentally, pondering why wide spread application of PCR-based tests in bacterial diagnostics has been elusive and identified a couple of key features that limit their use. It seems appropriate to start the new year with a discussion on one technology that can address those limitations – Infrared-based identification (IR).
What, you might be wondering, – that dilapidated instrument I vaguely recall using in undergraduate chemistry lab? Well, not quite that instrument but yes, one that utilizes the same fundamental principles.
The concept of using IR for identifying bacteria is not new. The earliest reference that we have been able to find dates back to 1950s! But, instrumental and computational limitations held back the potential for using this technology for identifying bacteria until the early 1980s. Naumann and colleagues took advantage of computational advances to demonstrate the ability of this technology to identify bacteria rapidly. Since then the use of IR for rapid and reliable identification of microbes to the strain level have been well documented. Reference databases to facilitate rapid identification of microorganisms are already available with some containing as many as 7000 strains.
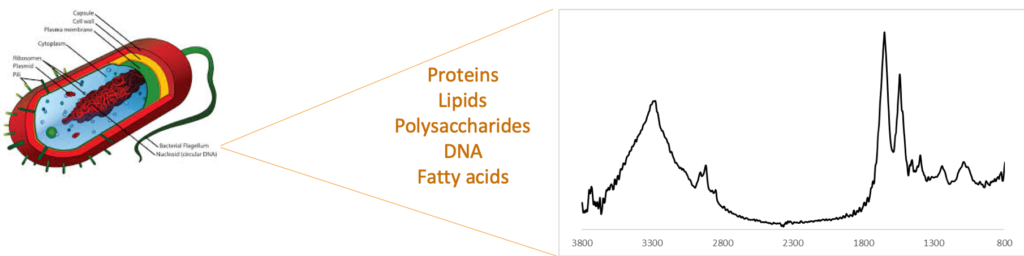
How does the technology work? IR, as you may recall, is a widely used vibrational spectroscopy technique that is used to identify compounds, even those present in mixtures. It is routinely used in raw material testing in the pharmaceutical and other industries as well as in testing of milk and milk products. All of the components that make up a bacterium (proteins, lipids, sugars, etc.) contribute to an IR “fingerprint” (see figure below). The nature and concentration of these components differ from one strain to another resulting in unique IR-fingerprints. This bacterial fingerprint has been used to differentiate between multiple bacterial species and strains including differentiating between antibiotic-resistant and -susceptible strains.
Bacterial fingerprint obtained by Infrared spectroscopy. Each species and strain has a different composition and hence a unique fingerprint.
How does it compare to PCR-based identification? Two key limitations of PCR-based tests that we had discussed previously were clinical sensitivity of the test and cost per test. If a PCR-test yielded a negative result, the clinician would not have any actionable information. On the other hand, with IR-based identification, the profile of a bacteria is very distinctive and its absence clearly indicates the absence of bacteria in the sample. In such a case, the clinician can actively consider whether administering antibiotics will be of any benefit to the patient. In the case of a positive result, the actions are similar to that with a PCR-based test with several important benefits. These are:
the result is available in ≤ 10 minutes
No custom labels or reagents are needed lowering the cost per test
It does not require specialized laboratory for operation
The bacteria is intact and viable after the analysis
Antibiotic resistance can be determined
The number of species and strains that are identified can be easily expanded without requiring new primers or antibiodies. This is done as a software update that consists of the fingerprint of the new bacteria and adjustments to the recognition algorithm, if needed.
You might be wondering at this stage why, if IR has all these benefits, there has not been any IR-based commercial instrument for use in bacterial ID? There are commercial instruments from Bruker, Thermo, and others that are used for bacterial ID in food safety testing. However the methodology used today requires bacteria to be cultured prior to identification (i.e. the same as most PCR-based tests). In addition, the bacteria has to be separated from the matrix components in order to make an accurate ID. Owing to these reasons, the technology has not yet seen widespread adoption for clinical use.
It is this aspect that we have impacted with the development of our separation cartridge. As mentioned previously, our separation cartridge can isolate and concentrate intact bacteria directly from blood with minimal manual intervention. The isolated bacteria can be identified using any technique. Using it upstream of IR however, permits rapid and sensitive identification of bacteria directly from patient sample without using any bacteria-specific labels or reagents. This combination of our separation cartridge and IR-based identification will, we believe, permit rapid, inexpensive, and hypothesis-free detection and identification. We aim to demonstrate this in 2020.
As we have said before, it’s not that IR (or any other ID technique) has to wholly replace PCR-based tests. The problem is large enough that multiple solutions will be needed. But, given the history of limited gains in developing effective PCR-based bacterial ID tests, the more diagnostic options we have, the better we can aid physicians in making the best decisions for treatment while slowing the spread of antimicrobial resistant bacteria. IR-based identification presents a compelling case to be a key diagnostic option.
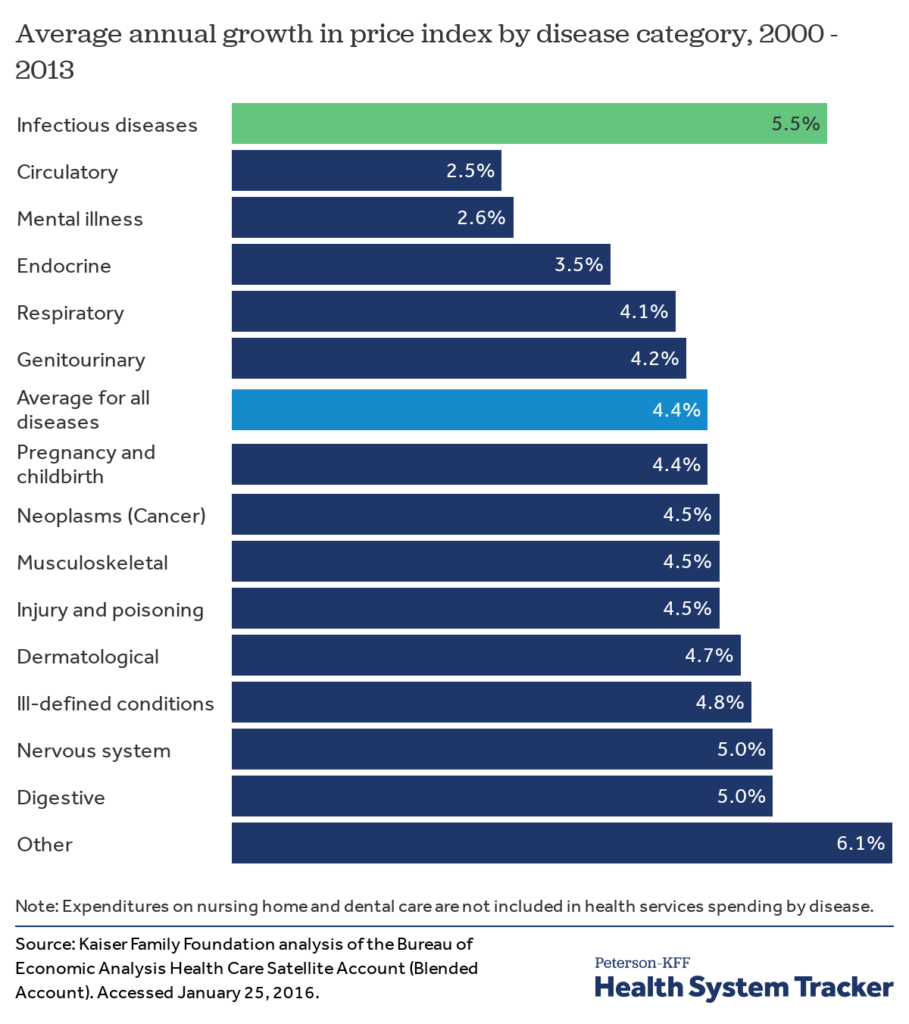
Antibiotics and focusing on infectious diseases is not the area where brainpower and money are focused on presently. It’s not as if people have suddenly stopped getting infections or that we don’t incur huge medical care costs because of them. Three infectious diseases were ranked in the top ten causes of death worldwide in 2016 by the World Health Organization. In the US, Among major disease categories, the cost per case grew fastest for infectious diseases.
Meanwhile the cost of treating patients who develop sepsis in the hospital rose by 20% in just three years, with hospitals spending $1.5 billion more last year than in 2015. In the US, the average cost per case for hospital-associated sepsis was slightly over $70,000 in 2018 with an annual increase in incidence of nearly 13%. Each year at least 1.7 million adults develop Sepsis and one in three patients who die in a hospital have Sepsis.
So, why the apparent lack of interest in tackling the problem? The challenges with new antibiotics development have been eloquently summarized by Isaac Stoner that I would highly recommend reading regardless of whether you are interested in this space or not. This captures the challenges faced by an antibiotic developer in achieving commercial success even if they have achieved technical success (i.e. a new antibiotic that works). Largely because of these struggles, many have concluded that antibiotics development carries too high a risk with very little return presently; one just has to wait until someone finds a way to make antibiotics profitable again.
Paradoxically, the situation, impact, and incentives work the other way for diagnostics. But this does not appear to have been fully appreciated by the broader audience yet. And recent “successes” have not delivered on expectations. But the case to persist is strong.
New antibiotics struggle to achieve commercial success because they are reserved for use as a last resort. This antibiotic stewardship, which is needed, limits the number of prescriptions for the new antibiotic making it difficult to achieve profitability. Having a diagnostic determine which antibiotic to administer (new or existing) promotes stewardship and reduces both overuse and misuse of antibiotics. If done right, the volumes of these tests would be sufficiently large (100 million tests in US alone each year) to assure profitability.
Diagnosis-related Group coding (DRG; where insurers pay a lump sum to hospitals for treatment) incentivizes hospitals to use inexpensive antibiotics, which places significant pricing pressure on new expensive antibiotics. But, it also incentivizes hospitals to get the initial antibiotic right since use of appropriate antibiotics early improves patient outcomes and reduces length of stay. i.e. hospitals get to keep more of the lump sum payment increasing their profit margins. In cases like Sepsis (which is one of the most expensive conditions to treat in hospitals), this makes a huge impact. It may even be the difference between whether the hospital is able to break even or not.
So, a well-designed diagnostic approach will garner strong stakeholder (patients, payers, society) support and command large volumes needed to be successful. It is difficult for antibiotics, with the healthcare and reimbursement models in effect today, to have such support or volumes.
Challenges
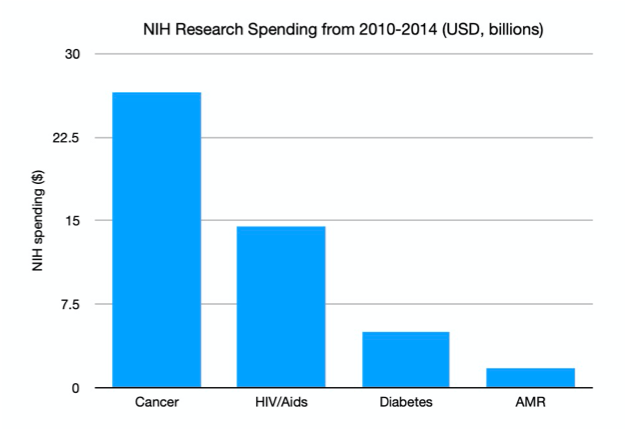
The one area where antibiotic development and diagnostics development share common ground is in investment attention – both struggle for it. Even well-intentioned programs like CARB-X and NIH grants do not devote sufficient funds for diagnostics development (see chart). While several governments, notably the UK, and the WHO have been campaigning for greater investment action, there are no moonshot initiatives to combat antimicrobial resistance. All this despite evidence that an appropriate diagnostic would allow us to dramatically improve the efficiency of existing drugs and buy us time to develop other long-term strategies.
Even though the market is huge, the impact is huge, and there is a real problem in need of a solution, limited resources (human and financial) have been devoted to this area and problem. So, we find ourselves in the situation today where there is no diagnostic that can help physicians determine if an antibiotic is necessary and which one to use. The core technology we use is effectively the same since the early 20th century!
This is partly because the approaches being attempted use the same basic strategy as those that have been tried before (that did not yield desired outcomes) with advances in technology incorporated. so, it is not too surprising that they have not yielded the desired results. The willingness to adopt a high-risk high reward strategy by investors as done in areas such as oncology therapeutics has been conspicuously absent. It’s not that investors are not aware of the challenges posed by AMR and Sepsis or the need for a solution. But, there needs to beat least one good commercial success story to renew the interest in this space. The high rewards are not readily apparent to investors burned by previous approaches. New, improved technical solutions and business models have not matured/been developed either. And this paucity of solutions is only made more difficult as talent seeks the security of better-funded areas.
They have been proposals to increase the economic incentives for developing much needed antibiotics. So far these well intentioned efforts have not resulted in some technical success but not the growth of self-sustaining companies. Pragmatically the success story is more likely to come via diagnostics (for the reasons outlined above) than in therapeutics. Or through a combination of diagnostic and therapeutic approaches enabling precision medicine for infectious diseases.
Progress
Despite these challenges, we are optimistic about the prospect of new innovative solutions and our platform, Biospectrix™. The ideal diagnostic should be able to detect the presence/absence of bacteria, determine its identity, and if it is antibiotic resistant – all in 15-60 minutes. Early results in our lab indicate that we can meet all of the above requirements.
With our approach, we aim to isolate, detect, and identify bacteria in < 1 hour without destroying the bacteria. The information from the analysis is utilized by the physician to administer the appropriate antibiotic. Through this process, patient outcomes will improve, length of stay in hospitals will decrease, hospital profit margins will improve, and, crucially, we can slow down the spread of antimicrobial resistance by cutting down on inappropriate antibiotic use. This is an outcome worth persevering for.
And, by the way, once we are done with our analysis, the bacteria can be cultured (from the sample we analyzed) and subjected to further analysis, if needed, but without the time pressure.
Enabling targeted therapy will permit new antibiotics being used judiciously as opposed to simply being saved as a method of last resort when it might be too late. Judicious use would provide the volumes needed for antibiotic developers to be profitable. It would also prolong the life of existing drugs. The possibilities for individual and societal good and commercial success are tantalizing. And that is why we believe that diagnostics are the place to start to combat AMR and Sepsis.
There is still some ways to go and many challenges to overcome before this vision becomes reality. But, we do so knowing that technical and commercial success with a positive impact on patients and healthcare, as we know it, is near. Jim O’Neil stated in his assessment on antimicrobial resistance, “One of the greatest worries about AMR is that modern health systems and treatments that rely heavily on antibiotics could be severely undermined.” We intend to do our part in preventing this bleak scenario from becoming reality.
For want of a nail, as the proverb tells us, a kingdom was lost. Would we lose the battle against the spread of antibiotic resistant bacteria for want of a better diagnostic?
The CDC notes that we are already in a “post-antibiotic” era. “Untreatable infections are no longer a future threat – they are a reality.” More than 2.8 million antibiotic-resistant infections occur in the United States each year resulting in more than 35,000 deaths. 223,900 people required hospital care for C. difficile. At least 12,800 people died in 2017 from these infections.
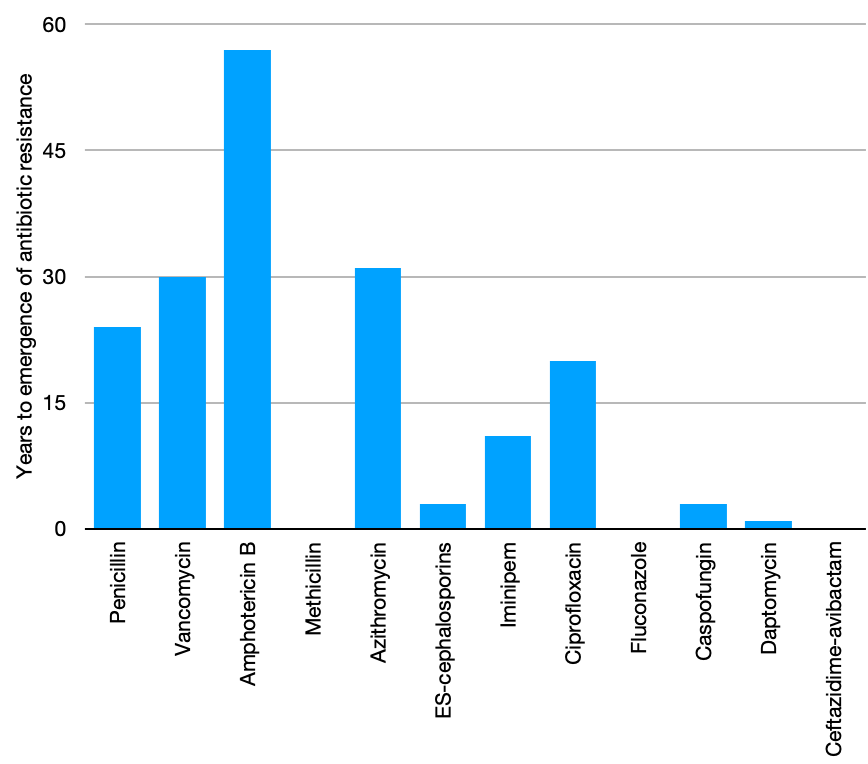
Relying only on new antibiotics as a solution is an ineffective strategy. Bacteria change continuously and develop new ways to resist antibiotics. Even a new antibiotic is effective only for a while before resistance emerges (see chart). The national plan to combat antimicrobial resistance calls for action in five core areas. One area is to ensure appropriate use of antibiotics. Better and innovative diagnostic tools are needed to achieve this goal.
In an era where DNA-based testing is seen as a solution for all identification needs, why is this approach not yielding the desired outcome? There are many reasons. One main reason is the absence of effective sample preparation approaches.
Components that interfere with DNA-recognition (e.g. human DNA) affect test accuracy. Current approaches do not eliminate these components effectively or rapidly. As a result, the test results are not dependable or timely. In other words, they do not ensure appropriate antibiotic use.
Test accuracy will improve if bacteria is isolated from the patient sample before analysis. The challenge is to do so efficiently and rapidly. Ideally, the procedure should isolate any bacteria and not just a small number.
This is where the recently introduced separation cartridge from 3i Diagnostics could be transformational. Intact and live bacteria is isolated easily, accurately, and rapidly (≤ 1 hour) directly from the patient sample using their cartridge and a syringe pump. The best part? It doesn’t matter what the bacteria is! The isolated intact and live bacteria can be easily identified using any technique. We will discuss the relative merits of the different bacteria tests in a future post.
Infection can be caused by a wide range of bacteria. One cannot identify the bacteria if it is not isolated in the first place. Hence, the ability to isolate any bacteria improves the dependability of the identification test. It also simplifies the test procedure and reduces cost per test. Many health research organizations are starting to evaluate the cartridge. Is it compatible with current clinical workflow? Does it improve accuracy of current tests? Does it help obtain results quicker? These are some of the question being asked by these studies. We will report on these studies when results become available
While we definitely need new antibiotics, existing ones still work. We however need to ensure that only those who need them receive them. Improved diagnostics will help slow the spread of antibiotic resistant bacteria and help preserve current and future, drugs. Sample preparation may not be as “cool” discovering a new antibiotic. But, in the effort to combat antibiotic resistance, it is just as important.